



Has Healthcare Bureaucracy Replaced Basic Human Decency?
In emergencies, hospitals, ICUs, and battlefields, the most in need go first. Why not in family medicine? Why The Healthy Keep Their Doctors While the Sick Wait in Line.


On The Way Home
In the shiny black rain of a busy highway at night you slow as you come upon cars twisted, lights crossed, and people panicked on the road. Heart racing you pull off the shoulder. You tell the kids to wait and not get out of the car. You hit your haard lights, and race to see the broken guardrail and three cars tangled precariously over the embankment.
Skidding down the loose gravel hillside you hear people yelling, in agony and despair. You’re not the first on the scene. Others like you are running toward the danger. One car in flames. Another angled such that it may fall over the hillside. The third on its crushed in roof.
It’s a night you will never forget. Your mind will return again and again to the choices you made, the effort you put in, and the risks you took. The commendation for brave conduct is framed on the wall, but not out conspicuously where others can see it. The narrative description is just a reminder for you; how you conducted yourself and what you’d do again just as unthinkingly as that night.
You helped the ones in the most immediate danger first. Then the ones in most need. And finally, you sat in the dirt and held a man you didn’t know as if he were your child. Comforting him not with words but with your body as his life ended in blood, tears, and curses. Cries for his mother that harmonized with sirens you began to hear high in the distance.
Though you would never have imagined it possible just an hour before; you did what any good and decent person would do. It’s shocking to look back at the long lists of history to see how many Nova Scotians through battles, war, disaster, emergency, and panic have done the same and more.
Triage
Triage is a word we most often associate with war, hospitals, and disaster zones. But in its essence, it is something much deeper—an ancient human instinct, a moral imperative, and a practical method for decision-making when resources, time, and the ability to save lives are stretched beyond their limits.
The word itself comes from the French verb trier, meaning "to sort" or "to select." It was first codified as a medical practice by Napoleon’s battlefield surgeons, who had to decide, in the chaos of war, who could be saved, who needed immediate attention, and who, tragically, would have to be left to die. But the concept is far older than its military origins. It is found in every moment of crisis where choices must be made—who gets the lifeboat seat, who gets shelter in a storm, whose voice gets heard first when all are screaming for help.
For many of the TV generation, triage was a central concept in MASH (the novel, film, and TV series), reflecting the reality of battlefield medicine during the Korean War. In the Mobile Army Surgical Hospitals, triage determined which wounded soldiers received immediate surgery, which could wait, and which were beyond saving. This system of prioritizing care based on urgency rather than rank or personal preference underscored the high-stakes, often chaotic environment of war medicine. It also served as a dramatic and thematic device, highlighting the ethical dilemmas, emotional toll, and dark humor that defined the series' tone.
At its core, triage is a test of our values. It is about fairness, necessity, and duty. It forces us to ask: What is the best course of action when all courses are tragic? In moments like the one on that rain-slicked highway, it is not a calculated policy but an instinctual human response—an automatic sorting of need, urgency, and possibility. It is an ethic of care in its rawest form.
For Nova Scotians, the history of triage is written in a history book of disaster, heroism, and hardship. In the aftermath of the Halifax Explosion in 1917, doctors and nurses, many barely trained, were forced to make brutal decisions in makeshift hospitals, using colored tags to classify the wounded. During the Titanic rescue efforts, it was Nova Scotia’s ships that arrived to recover survivors and the lost, deciding who could be saved from the freezing Atlantic. In every storm, fire, shipwreck, and crash, the question has been the same: Who needs help the most, and who can still be saved?
Triage is not just a medical or emergency response system. It is a philosophy of prioritization that runs through every aspect of human life—leadership, economics, politics, and even daily choices. We practice it in small ways every day, deciding what deserves our attention, our time, and our effort.
But in its purest form—when life is on the line—it reveals something fundamental about who we are. Not just as individuals, but as a people.
The Healthcare System
If you are bleeding out in an emergency room, the system kicks into high gear. The triage nurse assesses you, prioritizing your care over the man with a sprained wrist or the teenager with a mild fever. That’s how medicine works—or at least how it’s supposed to work. In war, in disaster zones, in ICUs, on organ donation lists, the same principle applies: the sickest, the most vulnerable, those at greatest risk, go first.
That is not just efficiency—it is morality. It is how any reasonable, ethical society distributes life-saving care when there isn’t enough to go around.
Except when it comes to family doctors.
Here, in the realm of primary care, where the stakes are lower but the access is supposedly universal, we abandon that morality completely. Instead of prioritizing the sick, we distribute doctors based on blind bureaucratic inertia. If you were lucky enough to get a doctor twenty years ago, you’re set. If you move to a new town? Too bad. If you’ve been healthy all your life but now desperately need care? Get in line with everyone else. Nova Scotia, where over 100,000 people languish on a waiting list for a doctor, operates on a system that is not just broken, but morally indefensible.
You Can’t Do That Here
A couple of things happened recently that I won’t get into except to say that it put the thought in my mind that I should give up my family doctor and give my place to someone who I can see clearly needs it more.
So, not really knowing where to start with that, I called and booked an appointment with my doctor. “Did I need to see her in person?” the booking agent asked. “No.” This was early October. The phone appointment was set for the earliest possible date… January 12th.
When the Doctor called, she was pleasant enough. We’d really only met once in an introductory appointment after my doctor of thirty-plus years retired and recruited, somehow, this replacement.
I made clear this wasn’t a medical call and plainly stated my plan: I’d like to swap out for someone I know who needs a doctor more than me. There was silence. Basically she said, that’s not a thing. It didn’t feel like a negotiation or discussion, and she clearly did not have the authority to even speak to the idea.
It’s one of the central tenets of bureaucracy. Only experts, those with power and control, are in a position to know and act. Everyone else is a fool, doesn’t understand, and is a threat to the rules and the system.
I could tell the doctor was not comfortable with this line of talk. She had no more power here than I did. I thanked her. Hung up. And dove into researching. It’s not often you stump the internet. Apparently, this isn’t a thing anyone has wondered too deeply about.
I went back to learn what I could about how the LIST actually works. The Need a Family Practice Registry in Nova Scotia is designed to connect residents without a primary care provider to available family doctors or nurse practitioners:
Registration Process
How to Register:
Online: Visit the official registry website and complete the registration form.
By Phone: Call 811, available Monday through Friday from 10:00 a.m. to 6:00 p.m.
Health Questionnaire: As of June 22, 2023, registrants can voluntarily add health information to their profiles. This data helps match individuals with appropriate services and care options in their community.
Assignment to Primary Care Providers
Standard Matching Process:
Community-Based Lists: Registrants are organized by community and listed chronologically based on their registration date.
First-Come, First-Served: When a primary care provider in a community is available to take new patients, they receive the list of individuals in that area and typically select patients starting from the earliest registrants.
Health Needs Consideration:
With the introduction of the health questionnaire, there's potential for prioritizing patients based on medical needs. This means individuals with more urgent health concerns might be matched with providers sooner, though the exact implementation details are evolving. It is not knowable by the public how or if this is done or how much.
Incentives for Physicians
To encourage the acceptance of patients with higher needs, Nova Scotia introduced an incentive program:
Financial Incentives gameify the system: Eligible family doctors receive $10,000 for accepting 50 high-needs patients from the registry, with an additional $200 for each extra patient accepted within a specified timeframe.
Current Statistics
As of January 2, 2025, there are 110,456 Nova Scotians on the registry, accounting for approximately 10.4% of the province's population. It’s really important to understand this is NOT the number of people without a doctor - this is the number of people who have become aware of the list and chosen to put their name on it over the years since it was created.
CBC’s most recent investigation into the latest numbers on the percent of Canadians who have a doctor looks more like this:
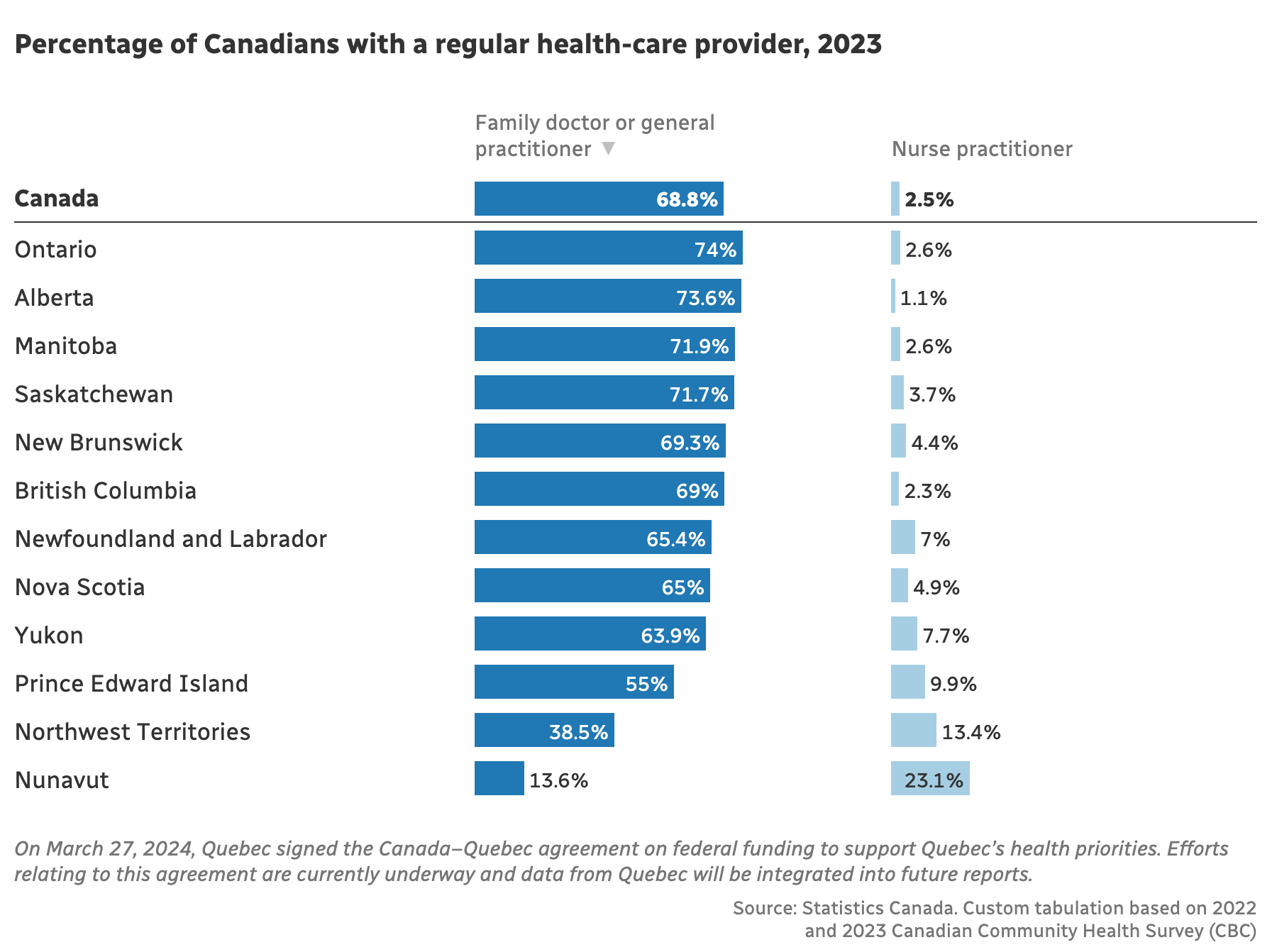
Statscan’s latest 2023 figures reveal, 5.4 million (17 per cent) Canadians aged 18 and older didn't have access to a regular health care provider, such as a family doctor, general practitioner, medical specialist or nurse practitioner, according to the report. It’s likely Nova Scotia’s number, if known, would move toward that number.
First Come - First Serve
In summary, the registry primarily operates on a first-come, first-served basis within each community. However, recent changes aim to incorporate health needs into the matching process, and may eventually ensure those with more urgent requirements receive timely care. But the truth is no one knows how it actually works. It’s a deeply bureaucratic black box that we are asked not to question.
I have enough experience with stuff like this to know how hard anyone questioning the system would be pushed back against.
So here’s my list of likely arguments against people charitably giving up their doctor if they knew their place would be given to a needy person.
1. It Would Undermine Fairness in the System
Allowing swaps could privilege those with social networks, family, and friends over people with greater health needs but fewer connections.
2. It Could Be Exploited or Monetized
A black market for doctor swaps could emerge, where people charge money or offer favors to "trade" their spot.
This could be especially problematic given the doctor shortage—people might start selling access to doctors instead of it being based on need.
3. Doctors Need to Choose Their Patients
Family doctors aren’t just random service providers; they build long-term relationships with patients.
If patients could swap themselves out, doctors could end up with patients they wouldn’t have chosen—perhaps with complex needs beyond their scope or workload capacity.
4. It Undermines the Purpose of a Public Healthcare System
Canada’s healthcare system is designed to allocate care based on need, not personal transactions.
If people can start "giving away" medical spots, it creates a two-tiered effect where access depends on who you know, not what you need.
5. It Would Be Logistically Messy
Who tracks and approves swaps?
Would it require paperwork, government approval, or doctor consent?
If someone swaps and then regrets it, does the system let them swap back?
In short, while it’s an empathetic idea, the risks of unfairness, exploitation, and logistical nightmares outweigh the potential benefits. The province instead relies on waitlists and a first come first serve take-a-number type bureaucracy… that is now, in theory beginning to add other choosing rules, though those rules, who makes them, who implements them, and who does the choosing are unknown and unknowable in our bureaucratic system. Without transparency, accountability, or clear lines or responsibility… well, we just don’t know anything.
The Perverse Incentives of Primary Care
It is remarkable that a system designed to care for people can become so completely detached from the principles of care itself.
Instead of a structure where doctors serve those who need them most and citizens have the right to decide, we have a bureaucratic system where personal physicians are handed out like property deeds—claimed, owned, and held onto for life. The implicit assumption of ‘the list’ is that every single person, at every moment, requires their own dedicated doctor, regardless of their health status. This is a relatively new expectation in human history, one that is increasingly difficult to meet.
When I was a kid, it seemed like we were doing well in Nova Scotia when every town or county had a doctor. Now the expectation is that every single person has a personal physician. That’s a tall order, something never imagined in all of history. How this is supposed to work and how it gets paid for is a work in progress. Wouldn't it be simpler to just ensure that everyone who NEEDS a doctor has one, and other more generally healthy people... meaning most of the population… offer “their's” up to help.
The more logical—and ethical—approach would be to recognize that access to a doctor should be dynamic, not static. If a generally healthy person has a family doctor, but their brother—who is chronically ill, has blocked arteries, is nearly blind, or is in constant pain infection due to tooth decay—does not, then why should the healthier sibling keep their place in line? If a healthy grandfather wants to pass on their place in line to a 3-year-old granddaughter who is struggling and Mom needs some help with consistent care, wouldn’t that feel… right? In an actual hospital, they’d be prioritized. In an organ transplant list, the most in need would go first. In any rational system of care, their need would outweigh someone else’s unused convenience. But in primary care, this kind of moral consideration simply does not exist.
The Bureaucratic Mind vs. The Moral Mind
The problem is that healthcare, particularly primary care, is no longer treated as a human relationship between caregivers and those in need. It has been swallowed whole by bureaucracy. And bureaucracies have no moral compass—they only have rules.
In emergency medicine, rules are designed around ethics: saving the most lives, helping the sickest first.
In primary care, rules are designed around paperwork and lists: assigned patient lists, long-term retention, bureaucratic stability, structure, and heirarcy.
The result is a system that fails to serve those who need it most. The absurdity is staggering. If a disaster struck, Nova Scotia’s doctors would immediately triage, shifting their attention to those in the worst condition. Yet in everyday life, those very same doctors are locked into seeing patients who might not have needed an appointment in years, while thousands with pressing conditions go without care at all.
How is this not a scandal? Why is no one talking about it this way?
The Scarcity Myth and the Culture of Fear
One reason is that in times of acute crisis—war, pandemics, mass casualty events—people rise to the occasion. They give up their place in line. They donate blood, volunteer, and offer up whatever they can. But in slow-motion crises, like the doctor shortage, people do the opposite: they hoard, they dig in, they protect what they have. This is the other perverse effect of our system: it conditions people to see healthcare as an individual entitlement, rather than a shared public good.
It is telling that Nova Scotians, among the most charitable people in Canada, have never been given the opportunity to voluntarily step aside for someone in greater need. If there were a formal way for people in good health to transfer their doctor to someone without one but in real need, how many would? It’s impossible to say—because the system refuses to even ask the question. But I have a pretty good idea. Tens of thousands. People would be lining up to do it, if they knew their sacrifice was for the good of someone in need.
Let’s Talk About Nova Scotia Charity
Nova Scotia is not a place; it is a promise—a quiet, unwavering vow etched in salt and stone, right in the bones of those who call it home. Here, generosity is not a choice but a reflex, as natural as breath. Nova Scotians are of the ancestors who ran toward the bullets, into the fire, into the storm, never hesitating, never needing to be asked. When ships go down in the black winter sea, we launch into the waves. When tragedy strikes, we gather, arms open, kitchens warm, hearts vast enough to hold the grief of others as our own. Ours is a land where men rowed into the Halifax Explosion, blinded and burned, to save strangers; where women stitched and fed and sheltered without question; where entire villages have emptied into the search for a single lost soul. The sacrifice here is quiet—never for show, never for reward—just the simple, unshakable instinct of a people who know that when the worst comes, you stand, you help, you give. Over and over again we see it when the cauldron of tragedy flames up. And when the world forgets, we still remember. Because that is who we are. That is what we do. That is Nova Scotia.
The Hardest Truth: Not Everyone Needs a Doctor—But Some People Desperately Do
Here’s the uncomfortable truth: not everyone needs a dedicated family doctor at all times. Many people go years without visiting one. Meanwhile, others—people with multiple chronic conditions, disabilities, or deteriorating health—live in medical limbo, bouncing between walk-in clinics, emergency rooms, and telehealth services.
What if we flipped the model? What if we recognized that doctors should be assigned based on actual medical need, not historical accident? What if we allowed fluid movement, where healthier individuals deferred their spots in the system to those in crisis, with the understanding that when their time of need came, someone else would do the same for them?
Would that be more efficient? Perhaps. But more importantly, would it be more just?
Absolutely.
The Real Question No One Is Asking
The real conversation isn’t about doctor shortages. It’s about whether primary care should operate on the same moral principles that guide every other aspect of healthcare. And that an accountable, transparent moral code and clear lines of responsibility should be a guiding light that all can see… and be proud of. Emergency rooms don’t operate on a first-come, first-served basis—so why do family doctors? Organ transplants aren’t given out by lottery—so why are family doctors assigned by historical inertia? If we accept triage as the highest ethic of medicine everywhere else, why do we abandon it, or make it a secondary consideration, when it comes to primary care?
This is not just an administrative failure. It is a moral failure. Perhaps the greatest of our time. And until we reframe the conversation—not just as one of inefficiency, but of injustice—nothing will change.
And people will continue to suffer, not because care doesn’t exist, but because we are not doing the right thing.
The solution is simple but unpleasant
We have to push everything to the front lines. All the money, technology, tools, labor—every resource we have—must move to where the need is greatest. The best people should be in collaborative care, guiding patients through emergency rooms, and even making house calls. No one wants to be in the trenches, but that’s where the real fight for healthcare happens. If we want a system that truly serves people, we have to stop building barriers and start bringing care to them.
Bureaucracy grows naturally, like a creeping vine, pulling resources and talent away from where they’re needed most. It’s human nature—given the choice, people will seek comfort, predictability, and status over the stress and exhaustion of the front lines. Administrators multiply, middle management expands, and soon, the system exists more to sustain itself than to serve patients. The only way to reverse this is with a military mindset—one that prioritizes the mission above all else. Just as in battle, the best leaders and resources must be deployed where the fight is happening, not tucked away in offices, meetings, or layers of approval processes. This requires a moral imperative—a collective commitment that healthcare is about serving patients first, not protecting bureaucratic turf. To make this shift, we need policies and incentives that pull doctors, nurses, and support staff forward, rewarding those who show up where they’re truly needed and resisting the gravitational pull of administrative bloat. Without this kind of discipline, healthcare will remain what it’s becoming—a fortress of paperwork, where the real fight for care is buried under layers of delay.